Variations in bundling by payer lead to claim reimbursement losses that most practices never realize. An unremarkable claim can be labelled "processed as bundled," with no apparent reasoning, and slowly snowball into a shortfall. It is essential to understand how each payer 'bundles' services not only from a perspective of maximizing claim reimbursement but also compliance because improper unbundling (or "unbundling fraud") can lead to audits and penalties under CMS or other payer compliance programs.
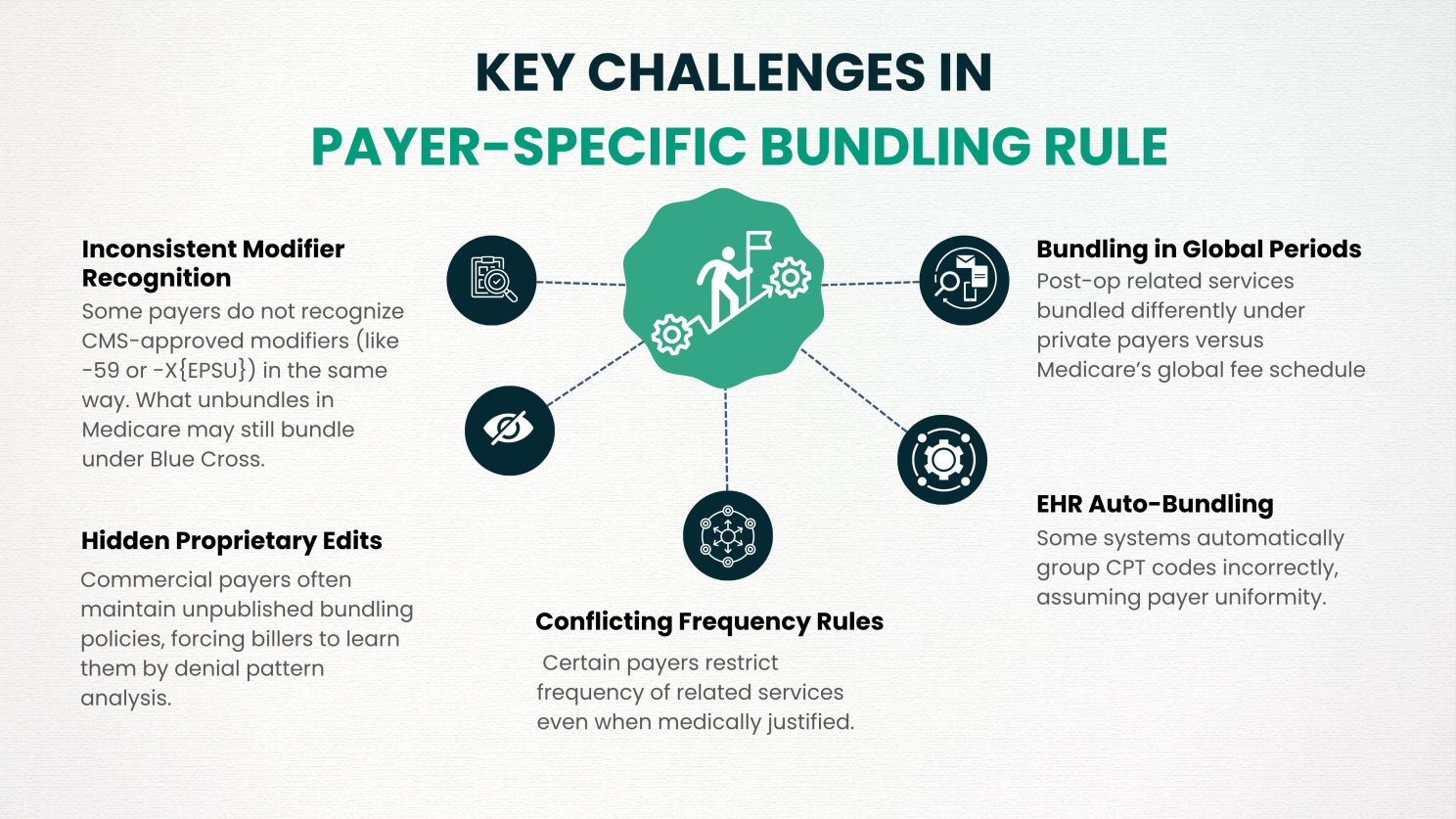
Hidden Proprietary Edits: Commercial payers often maintain unpublished bundling policies, forcing billers to learn them by denial pattern analysis.
Inconsistent Modifier Recognition: Some payers do not recognize CMS-approved modifiers (like -59 or -X{EPSU}) in the same way. What unbundles in Medicare may still bundle under Blue Cross.
Conflicting Frequency Rules: Certain payers restrict frequency of related services even when medically justified.
EHR Auto-Bundling: Some systems automatically group CPT codes incorrectly, assuming payer uniformity.
Bundling in Global Periods: Post-op related services bundled differently under private payers versus Medicare’s global fee schedule.
Still a must for reimbursement of claims from Medicare and Medicaid, specifying which CPT/HCPCS codes cannot be billed on the same claim.
Each payer builds its own bundling engine from utilization data and cost-containment algorithms, which introduces variation in claim reimbursement that billers must monitor independently per payer.
New mandates transparency laws from payers (2024–2025) require payers to disclose, on remittance advice, the rationale for bundling, but these mandates are often weakly enforced, leaving the provider community with a limited view of decisions related to claim reimbursement.
Providers maintain their right to appeal bundled denials, as well as all other denials, under CMS and state insurance laws, provided clinical opportunities exist that support separate claim reimbursement.
Track denials by payer and code combination to identify bundling trends that are suppressing claim reimbursement.
Identify whether the bundling is payer-specific or based solely on NCCI before appealing reduced claim reimbursement.
Each service rendered must be documented at the time of service and, where necessary, with diagnosis codes that support separate services to ensure they can be fully reimbursed on the claim.
Use -59, -25, or X{EPSU} as justified, not automatically. One of the surest ways to lose out on claim reimbursement is incorrect modifier use.
Advisory organizations tend to update their payers’ policies quarterly, and the bundling logic changes overnight without notice, directly affecting carry-forward claim reimbursement.
Commercial payers are often out of line with CMS; thus, billers must understand both systems to consistently shield claim reimbursement across all payer types.
Use medical necessity, time spent, and payer policy contradictions to overturn inappropriate bundling and recover lost claim reimbursement.